
NASAL AERODYNAMICS and RHINOSINUSITISES
Relationship between two parallel respiratory structures in the nose
The main cause of the night snoring is violations of the nasal aerodynamics
The functionality of the small ostiums of the nasal sinuses
The real significance of the limen nasi
VARIANTS OF NASAL AERODYNAMICS
NORMOGRAM OF NASAL AERODYNAMICS
PHYSIOLOGICAL BRIDGE REPRESENTED BY THE NASAL VALUE
SURGICAL RECONSTRUCTION OF NASAL AERODYNAMICS
SEPTOPLASRY UNDER CONTROL OF NASAL AERODYNAMICS
CONTRAINDICATION TO SEPTOPLASTY
PROTECTION OF THE LOWER MEATUS FROM INSPIRATION
THE INSIDIOUSNESS OF THE UNILATERAL "SOUTHERN" NASAL AERODYNAMICS.
The general aerflow passes through the lower nasal passageway and, as a result of the overloading of the nasal mucosa, it could be the cause of opened-mouth breathing, under effect of the unconditioned reflex
 |
Snoring at the saved nasal respiration.(IFOS,Sept.28-Oct.3,2002,Cairo, Egypt.) | |
ABSTRACT:It is known, that about 25% of the snoring people have saved nasal respiration, that hampers realizing of the cause of snore for them. The experience of utilizing of new data about nasal aerodynamics gave us the additional opportunity to research these patients and from this side. For instance, the "southern" type of nasal aerodynamics (STA) leads to overloading of the inferior meatus owing to the cold and dry air, that provokes dryness, itch, irritation, trauma and inflammation of the nasal mucosa. Such sensations and disturbances in the patient's nose with the STA could be provoke to the opened-mouth respiration at night, under influence of the unconditioned reflex. So, we determined nasal aerodynamics in 200 snore patients, who had no evident difficulties of nasal respiration and it was defined, that all of them had the STA. But, only 20 % admitted, that they kept the mouth breathing at night. Rhinoscopy let to reveal the irritation of the atrophic and dry mucosa into the inferior meatus and nasopharynx with signals of the inflammation. After fortnight anti-inflammatory therapy of the nasal and nasopharynx mucosa with protection of theirs from overloading, the reducing of dryness and itch into the nose and nasopharynx was noticed, with the snoring stopped in 52%. The surgical reconstruction of the STA into the "northern" type was made in 32 cases with follow-up termination of the snoring for an year and more. Introduction:Well-known fact, that from 10 % to 30 % of adult population suffers from snore [1,2]. At the same time, in the etio-pathogenesis and therapy of this disease there are many questions. For example, at present day, all recognize the snoring mechanism as a result of vibrations of the soft palate and root of the tongue upon inspiration through the mouth. The using of opened-mouth respiration owing to the difficult respiration through the nose under influence of the unconditioned reflex, that what fact is not call of disputes, too. Actually, it is common knowledge, that after restoration of nasal respiration the snoring is terminated, as a rule. Therefore, difficult nasal respiration is considered as a cause of the snore. And also, it is known fact, when the saved nasal respiration is met up in 25 % of the snoring people [3,4]. Such cases become very difficult for understanding of the cause of snoring. And with all this going on, the convincing explanation about this contradiction in the world bibliography we did not find out. New data of nasal aerodynamics (1995-1998)[5,6] assisted us to realise the cause of snoring for the patients with absence of nasal respiration difficulties. For instance, as it was established, that the overloading of a lower nasal passageway because of the cold and dry air was typical for the "southern" type of nasal aerodynamics (STA) and provoked dryness, itch, irritation, and trauma of the mucosa with development of inflammation, especially at night. And so, such overloading of the nasal mucosa, at the time of sleeping, could be as the cause of opened-mouth breathing, under effect of the unconditioned reflex, like owing to the difficulties of nasal respiration (Fig.1). For argumentation of such possibility, the type of nasal aerodynamics of snoring people with saved nasal respiration was necessary to clear up.Materials and methods:Under our observations were 200 snoring people with absence of evident difficulties of nasal respiration. They were at the age of 20 to 60, females and males were about in equal. These patients suffered because of the snore from 2 and over 20 years. Besides of common ENT survey, the type of nasal aerodynamics was investigated to all patients by means of the endonasal rhinomanometry with ours device of the intranasal rhinomanometry (Russian patients NN 1572505; 1602472). [6] with accuracy in 25 Pascal (Pa). For helping to these patients, medicinal and surgical correction of nasal aerodynamics infringements were produced with examination of their clinical appearances and snoring's dynamics as before and after treatment.Results:After testing of the nasal aerodynamics type we got the first acknowledgement of the snore dependency from the SNA, because it was established that general airflow at inspiration passed through IM under negative pressure from 175 to 200 Pa. Such data were typical exactly for the STA. This result confirmed, that our patients had the typical for STA feelings in the nose and nasopharynx at night and so, these sensations, under effect of the unconditioned reflex, could compel the patients to the open mouth respiration. 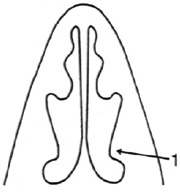 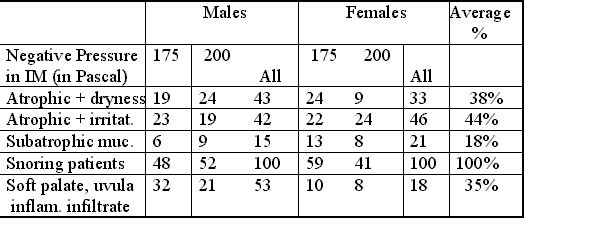 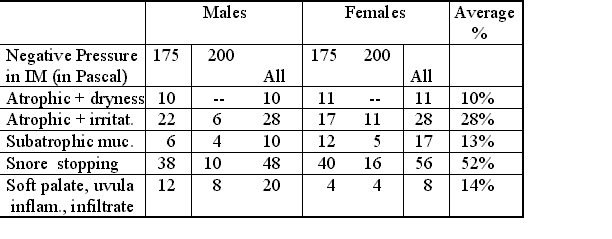 Conclusions:1. The basic cause of the snoring for the patients with saved nasal respiration is the "southern" type of nasal aerodynamics, which programs overloading of the nasal and nasopharynx mucosa and provokes the opened-mouth respiration at night under unconditional reflex. 2. The protection of the nasal and nasopharynx mucosa from overloading and anti-inflammatory therapy allow to stop the snoring for the each second patient with the saved nasal respiration. 3. The surgical reconstruction of the "southern" type of nasal aerodynamics into the "northern" one allows to end the snor for the patients with saved nasal respiration. References:[1] Chumakov F. About snore and stopping of a respiration in dream. J.Vrach, 1998;12:22-3. (in Russian) [2] Cit- Jay F. P, George A. G, , Donna L. W. and Kenneth B. S. Obstructive sleep apnea treatment outcomes pilot study. National Commission on Sleep Disorders Research. Otolaryng. HNS 1998;118(6):833-44 [3] Ilium P. Septal deviation in snoring patients evaluated by acustic rhinometry. 15th Eropean Rhinologic Congress, 13th ISLAN. Abstract Book. Copenhagen 1994; 125. [4] Mynin Y. The anatomic-physiological features of the upper respiratory ways for patients with snoring and obstructive sleep apnea in dream. XV Congress Otolaryng Russia. St. Petersburg.1995; 2:132-6. (in Russian) [5] Uliyanov Y.P. Surgical reconstruction of nasal aerodynamics. XVI World Congress of Otolaryng. HNS. Sydney.1997, p. 1591-5. [6] Uliyanov Y.P. Clinical manifestations of the Variants of the Nasal Aerodynamics. Otolaryng. HNS 1998; 119: 2: 152-3.
|

