
Caption:
The deviation of nasal septum or thorn of nasal septum makes unilateral "southern" nasal aerodynamics. Legends:NASAL AERODYNAMICS and RHINOSINUSITISES
Relationship between two parallel respiratory structures in the nose
The main cause of the night snoring is violations of the nasal aerodynamics
The functionality of the small ostiums of the nasal sinuses
The real significance of the limen nasi
VARIANTS OF NASAL AERODYNAMICS
NORMOGRAM OF NASAL AERODYNAMICS
PHYSIOLOGICAL BRIDGE REPRESENTED BY THE NASAL VALUE
SURGICAL RECONSTRUCTION OF NASAL AERODYNAMICS
SEPTOPLASRY UNDER CONTROL OF NASAL AERODYNAMICS
CONTRAINDICATION TO SEPTOPLASTY
PROTECTION OF THE INFERIOR NASAL PASSAGE FROM INSPIRATION
THE INSIDIOUSNESS OF THE UNILATERAL "SOUTHERN" NASAL AERODYNAMICS.
SNORING WHEN NASAL RESPIRATION IS SAVED
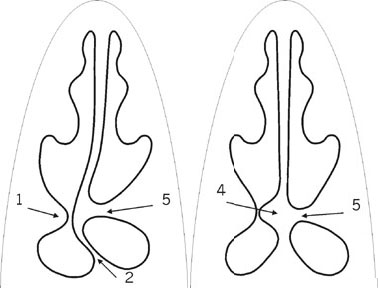
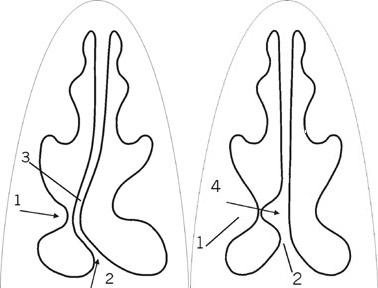
Caption:
The surgical reconstruction of the "southern" nasal aerodynamics into the northern type. Legends: |
Septoplasty under control of nasal aerodynamicsUlyanov Y.P. The XYII World Congr. of Otorhinolaringology.(IFOS,Sept.28-Oct.3,2002,Cairo, Egypt.) |
|||
ABSTRACT: 116N-oIt is common knowledge, that surgical correction of nasal septum deviation is keeping the leading place in nasal surgery, because this intervention influences on the both halves of the nose. At the same time, any smallest inaccuracies or mistakes in performing of septoplasty may negative exert upon nasal function. New data about nasal aerodynamics found out additional danger of mistakes in septoplasty, because the "northern" type of nasal aerodynamics (NTA), which is well adapted for any adverse climatic zones, could be destroy into the "southern" type (STA) with underdeveloped protective mechanisms, which reduces protective properties of the nose and can not reconstruct the "northern" on the other side (Y.P.Uliyanov, 1996-1998). Therefore today, the classical recommendations to septoplasty about only improvement of nasal respiration and criteria of its efficiency are needed in correction. So, we checked up nasal aerodynamics in 200 patients with chronic nasal obstruction due to septal deviations, and therefore, septoplasty was offered to them. In 156 cases the real recommendations to septoplasty were in principle differed from the traditional, which could destroy the NTA into the STA and so, reduce protective properties of the nose. That is why, we selected septoplasty fitted for saving the NTA, designed and used "partial septoplasty" and transformed the STA into the "northern" one. The good results were achieved, because the patients had got the NTA on the both nasal halves.Introduction:Since the papers of Fugall (1882), surgical correction of the deformed nasal septum has kept the leading place in surgery of the nose, because this intervention influenced on both halves of the nose, at once. On the other hand, any smallest inaccuracies or mistakes in performing of septoplasty may exert negative influence upon nasal functions of both halves, too. Therefore, rhinologists are constantly searching the most sparing and effective methods of septoplasty. However, existent multitudes of nasal septum deviations make extremely difficult selection of the suitable variant of septoplasty from large quantity of standard methods. Therefore, at present, the classical methods of septoplasty retain their value only as a reference book [2],[3]. Nevertheless, in every concrete case, rhinologists try to choose the best variant of intervention, and so, any new knowledge about nasal function is helping them. In this connection, the recent data about two functionally opposed types of nasal aerodynamics are the most important. The "northern" type of nasal aerodynamics (NTA) with expressed protective mechanism against the "harsh" (cold and dry) air is so effective, that such patients are well adapted to any adverse climatic zone. And the "southern" type of nasal aerodynamics (STA), which have underdeveloped protective mechanisms is suitable only for a "soft" air of southern latitudes like Mediterranean [4],[5],[6]. At the same time, as it turned out, the deviations of the nasal septum (NS) often made the NTA on a side of the nose and then, standard septoplasty could deform its into the STA, that destroies the protective mechanism of nasal aerodynamics and besides, it can not reconstruct the "northern" type on the other side. Consequently, today, the classical tasks for septoplasty and the criterions of its efficiency about only improvement of nasal respiration already are not enough longer, and they are needed in the additional correction for do not destroy the NTA and reconstruction of the "southern" type into the "northern" on the other side.Patients and methods:We examined 200 patients with chronic nasal obstruction due to septal deviation, to whom septoplasty was recommended by previous ENT specialists and these persons were directed into our clinic for surgical help. The age of the patients was from 16 to 37 and males were 123. The test of nasal aerodynamics was included into the complex of standard inspections of nasal disturbances. And so, to all patients, after removal of the nasal mucosa edema, the testing of nasal aerodynamics was carried out by the device for endonasal rhinomanometry (Russian patients NN 1572505; 1602472) as before therapy, so and after. For the NTA was typical separation of the middle meatus from lower that directed the main airstream upon inspiration into the middle meatus (MM) under negative pressure from 150 to 200 Pascal (Pa.). This separation could be created by the contact of the inferior turbinate (IT) with NS or the thorn, crest of IT, their adhesion or by the "physiological bridge"[7]. The presence of the "physiological bridge", we determined by the distance between the anterior end of the IT and NS. When this distance was less than 1,.5-2 mm., the "physiologic bridge" was formed in this place.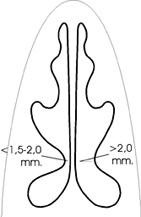 Results:After taking out the rhinedema, the compensated variants of nasal septum deviation with NTA on the both halves were detected in 18 patients. They had vasomotor rhinitis and so, were required in therapy for vasomotor edema. Two-side deformations of the nasal septum with obstruction of both nasal halves was found out in 31 patients (Group �), that was a basis to recommend septoplasty. For 18 from them (Group �-1) we selected fitted standard septoplasty to save the NTA, in 13 cases (Group �-2) we used "partial septoplasty" on the "northern" half (Fig.3), and additional reconstruction of the "southern" half into the NTA was performing to 7 patients (Fig.2) with overall positive result in 27. The unilateral nasal respiration was detected in 151patients with "southern" type aerodynamics on a side. Difficult respiration with expressed deformation of the NS to the "southern" half was found in 22 (Group B). For these patients we selected standard septoplasty fitted for saving the NTA with reconstruction of the STA into the "northern" one (Fig.2) on the other side and with well result. Expressed deformation of the nasal septum with difficult respiration on the "northern" half was detected in 58 from 151 (Group C) and for these patients we used "partial septoplasty" in 54 cases, while standard septoplasty for saving the NTA was selected in 4, and additional reconstruction of the "southern" half into the NTA on the other hand was done, with common good results in 49 cases. And the rest 71 patients from 151 (Group D) had well respiration only through the "southern" half of the nose, while, through the "northern" side breathing was good only, when the "southern" half was closed. Such one-sided respiration was depended of the shortest distance until the nasopharynx through the IM of the "southern" side, than along the MM on the "northern" half. This inevitably led to stagnant processes on the "northern" half that could form the false impression about its constriction. This erroneous impression was supplemented owing to the narrowing in the field of the "physiological bridge". In 27cases the "physiological bridge" was formed by the nasal septum deviations, by of its thorns (crests) in 20 cases and by a big size of the inferior turbinate in 21, and in 3 patients by the adhesions in this place. That what could induce the rhinologist to surgical intervention into this half of the nose for improvement respiration. We have paid attention, that if these deviations of NS, the thorns (crests) of NS or the big inferior turbinate to delete, the "physiological bridge" will be destroyed and then, the main airflow upon inspiration will fall into the IM, like in the STA, that will worsen protective properties of the nose. The real key to help to this patients was surgical transformation of the STA into the NTA (Fig.2). Such surgical reconfiguration of nasal aerodynamics was made in 63 patients from 71 (Group D) and with positive results in 51 cases. The good clinical result was accompanied by positive aerodynamical changes typical for the NTA. In the negative episodes, as a rule, the vasomotor disturbances in the nasal mucosa made difficulties of nasal breathing, and for these patients the further treatment for vasomotor disturbance was required. The real recommendations to septoplasty were in principle different from traditional in 156 cases (18 with NTA, 13 from Group A-2, 54 from Group C and 71 of Group D), because, the latters could destroyed the NTA into the "southern " type and could not transform the STA into the "northern" on the other side. The reconstruction of the "southern" type of nasal aerodynamics into the NTA was required in 158 patients (7 from Group A, 22 from Group B, 58 from Group C and 71 of Group D) Therefore nowadays, during all methods of septoplasty should be take into consideration the individual peculiarities of nasal aerodynamics, so that the nature protective mechanism of nasal aerodynamics will not destroy and the STA on the other side will.Conclusions:1. If the nasal septum deviation forms the physiological bridge, traditional septoplasty must not be done, not to destroy the already formed protective mechanism of the nasal aerodynamics. 2. When the thorn, crest of the nasal septum forming the physiologic bridge or adhesions in file of the physiologic bridge separating middle meatus from inferior one, it is inadmissible to remove them, not to destroy the protective mechanism of the nasal aerodynamics. 3. When the deformation of the nasal septum forms the "northern" type of nasal aerodynamics on one side and the "southern" type on the opposite side, to restore the protective function of the nose, surgical formation of the new air-directing "steering gear" is indicated on the "southern" side. 4. When the nasal septum is deviated near the physiological bridge, it is necessary to use partial septoplasty with shifting only medial and upper sections to retain the separating mechanism between the inferior and middle nasal passages. Fig. 3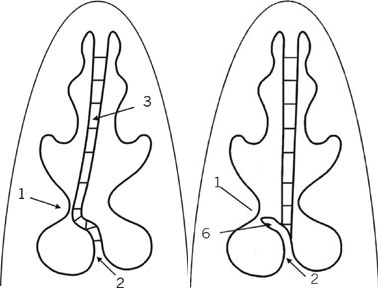 A BCaption:The partial variant septoplasty with shifting only the medial and superior parts of the nasal septum deviation (Russian Patent N 2141798). Legends: A. The nasal septal deviation was fragmented only in the medial and superior parts.B. The medial and superior parts of the septum movements to the centerline. References:[1] Fugall (1882) is cited of: FJ Stucker (1976). [2] Stucker FJ, Smith TE. Pitfalls in management of defects of bony dorsum and cartilaginous vault. Arch Otolaryngol 1976; 102: 695. [3] Stucker FJ, Ansel TE. A case against nasal packing Laryngoscope 1987; 88: 1314. [4] Uliyanov Y.P. Nose aerodynamics. Arch Otolaryngol Head Neck Surg 1995; 121: 352. [5] Uliyanov Y.P. Surgical reconstruction of nasal aerodynamics. XVI World Congress of Otolaryng. Head and Neck Surg. Sydney, 1997.p.1591-5. [6] Uliyanov Y.P. On Contraindication to Septoplasty. Otolaryngology-Head and Neck Surgery -August 1998; 119 (2): 153-4. [7] Uliyanov Y.P. Physiological bridge represented by the nasal valve and its variants. XVI World Congress of Otolaryng. Head and Neck Surg. Sydney, 1997.p. 1597-601. | ||||
|
|
||||

