
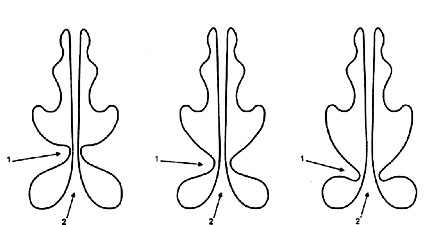
Fig. 2 The medium level type:
1 - inferior turbinate bone (with inclination of up to 15°);
2 - nasal septum.
Fig. 3
The lowest level type:
1 - inferior turbinate bone (with inclination of over to 15°);
2 - nasal septum.
NASAL AERODYNAMICS and RHINOSINUSITISES
Relationship between two parallel respiratory structures in the nose
The main cause of the night snoring is violations of the nasal aerodynamics
The functionality of the small ostiums of the nasal sinuses
The real significance of the limen nasi
VARIANTS OF NASAL AERODYNAMICS
NORMOGRAM OF NASAL AERODYNAMICS
PHYSIOLOGICAL BRIDGE REPRESENTED BY THE NASAL VALUE
SURGICAL RECONSTRUCTION OF NASAL AERODYNAMICS
SEPTOPLASRY UNDER CONTROL OF NASAL AERODYNAMICS
CONTRAINDICATION TO SEPTOPLASTY
PROTECTION OF THE INFERIOR NASAL PASSAGE FROM INSPIRATION
THE INSIDIOUSNESS OF THE UNILATERAL "SOUTHERN" NASAL AERODYNAMICS.

Fig. 5 Participation of the curvature of the nasal septum in formation of the physiological bridge:
1 - inferior turbinate bone of small size;
2 - curvature of the nasal septum in the direction of the inferior turbinate bone. ;
Fig. 6
Participation of compensatory hypertrophy of the inferior turbinate bone (when the nasal septum is curved) in formation of the physio-logical bridge:
1 - inferior turbinate bone with compensation through hypertrophy;
2 - curvature of the nasal septum in the opposite direction.
 |
Physiological bridge represented by the nasal valve and its variants(Uliyanov Y.P. Physiological bridge represented by the nasal valve and its variants. XYI World Congr. Of Otolar. Head Neck Surg.Sydney, Australia, 2-7 March, 1997: 1597-1601.) |
|||
SUMMARYTo register the data of the nasal aerodynamics characteristic of healthy subjects, we have examined 200 obviously healthy persons (age or sex were represented equally). With this aim in view, we have devel-oped a special device and a method for its application to study the air in the nasal passage. The main air flow during inspiration passed through the median nasal passage, whereas it passed through the inferior nasal passage in expiration. This redistribution was especially pronounced in 22% of the subjects examined. Twenty conventional units (CU) passed through the inferior nasal passage, 80 CU passed through the median nasal passage and 10 CU passed through the superior nasal passage. In expiration, 80 CU go through the inferior nasal passage, 20 CU through the median nasal passage, and 10 CU through the superior nasal pas-sage. This protective mechanism of the mucosa of the inferior nasal passage is likely to be especially important, as the mucosa of the nasal looked quite healthy: succulent, moist and pink.INTRODUCTIONRhinologists had spent a lot of effort before the physiological valve between the nasal septum and the anterior part of the inferior turbinate bone was detected. As far back as 1903, P.J.Mink drew attention to the valve mechanism in the nasal vestibule. Situated between the anterior parts of the nasal septum and the cartilagious framework of the external nasal wall, this mechanism exerts an important influence on the nasal respira-tion. This area of the nasal cavity has been called the nasal valve. S.Z. Piskunov (1993) was the most exact in determinating the site of the greatest functional load of the nasal valve. In his opinion, the nasal valve is situated several millimeters behind of the anterior part of the inferior turbinate bone at the narrowest area between the anterior parts of the inferior turbinate bone and nasal septum. However, it is here that intranasal cohesions, cicatricial synechiae, arise. Rhinologists have been engaged in dissecting the latter for many years, due to the fast that these synechiae persistently recur. Many meth-ods and instruments have been developed, including making a perforation in the nasal septum or removal of the inferior turbinate bbone [Altschuler M.A.,1945; Bokshtein F.S., 1956; Rauer A.E., 1936; Rosenfeld I.M., 1946]. However, there are no safe methods of removing the synechiae with-out extensive damage to surrounding tissues. As a result, E.B.Kern, T.D.Wang (1995) admit that an optimum methods of forming a mucosal flap to secure a success of surgery has not been found yet. These problems are to be considered and assessed at a different viewpoint after new data have been received during the studies of nasal aerodynamics according to our methods [Y.P.Ulianov, P.P.Polivanov, Rusian pat. №№1572595, 1602472]. These data have confirmed the correctness of the views of A.A.Atkarskaya (1925) and F.S.Bokstein (1956), despite discrepancy in their assertions. These authors described two extreme types of nasal aero-dynamics, which we call the northern and southern ones [Y.P.Ulianov, 1995]. The northern-type nose features the well-developed of the inferior turbinate bone which nearly reaches the nasal septum, with resulting direction of the air flow at inhalation into the medial nasal passage to be moistened and warmed before entering the respiratory ways. At exhala-tion, the main airstream goes through the inferior nasal passage, which results in formation of an area of the unmovable air column between the anterior boundary of the inferior turbinate bone and nasal septum, i.e. at the most narrow part of the nasal valve. This air column is a kind of physiological bridge does not take a direct part in respiration, but, in fact, participates, together with the inferior turbinate bone, in formation of the air-directing «steering gear» turning the airstream into the median nasal passage.PATIENTS AND METHODTo determine the variants of the physiological bridge formed by the nasal valve, we have examined 300 patients with physiological bridge. In patients of both sexes aged from five to 80 years, the distribution of these variants was approximately equal. Redistribution of air flows at inhalation and exhalation typical of the northern-type nose served as a criterion for establishing the existence of the physiological bridge. There main variants of location of the nasal physiological bridge as related to the height from the bottom of the nasal cavity could be demon-strated depending on the anatomical variants of the structure of the inferior turbinate bone. They are: the highest level, i.e. practically horizontal situa-tion of the inferior turbinate bone (Fig.1-1,2); the medium level, i.e. the situation of the inferior turbinate bone with an inclination of 10-15° (Fig.2-1,2); and the lowest level, caused by a sharp inclination of the infe-rior turbinate bone to the bottom with an angle of over 15° (Fig.3-1,2). In most cases (60%), the medium level was found. The lowest level was de-tected in 30% of cases, with the highest one being present in 10% of pa-tients. No age- or sex-related predilection was discovered. In relation to the tissues forming the physiological bridge, four anatomical variants can be established. The first one, which was men-tioned above, features the well-developed inferior turbinate bone. The second variant is marked by the lass-developed inferior turbinate bone and the oppositely situated ridge of the nasal septum (Fig.4-1,2,3). The ridges are more often than not two-sided. The third variant is charac-terized by the less-developed inferior turbinate bone, with the nasal septum approaching the latter while creating a curvature, permitting formation of the physiological bridge (Fig.5-1,2). There are reverse also rather frequent cases of the following variant: from the reverse side of the nasal septum, the inferior turbinate bone seems to try to catch up with the reclining nasal septum with enlarging in its size, which also makes it possible for the functional bridge to form (Fig.6-1,2). The first variant was found in 80% of cases, the second one in 10%, with the third, the forth and their combinations being detected in 4, 4 and 2%, respectively. The association between these main variations gives a sum of 12 ones. Besides, if various transitional forms and combinations with southern-type nasal aerodynamics from the other half of the nose are taken onto account, it becomes clear that an unambiguous determina-tion of the features of the nasal aerodynamics in each patient is not an easy matter, which means that the surgeon should «look before he laps». Therefore, rhinologists should reconsider traditional methods not to damage the delicate natural balance in the form of the physiological bridge represented by the nasal valve, which to a large extent control the health of our patients. Among the above-mentioned variants of formation of the nasal valve as the physiological bridge, one should pay attention to temporary conditions in the nose, i.e. transitional enlargement of the volume of the mucosa of the inferior turbinate bone and nasal septum resulted from the nasal cycle, vasomotor phenomena, inflammatory edema, etc. Spe-cial attention should be paid to the hypertrophic process of the mucosa of the inferior turbinate bone, which, being caused by a chronic in-flammatory process, seems to be subject to removal, but, at the same time, it forms the nasal valve as the physiological bridge, which is so much necessary for normal functioning of the nose. This is a topic for a special study, but these factors should be taken into consideration now in treating patients.REFERENCES1. Mink P,J, Lez comme voie respiratoire. Presse Otolaryngol. (Belg.) 1903; 481-96.2. Piskunov S.Z. Physiology and pathphysiology of the nose and paranasal sinuses. Rossiyskaya Rinologiya. 1993; №1: 19-38 (In Russian). 3. Altschuler M.A. On the techniques of eliminating intranasal synechiae. Vestnik otorinolaringologii. 1945: №1: 39-40 (In Russian). 4. Bokshtein F.S. Intranasal surgery. Moscow; 1956: 232 pp. (In Russian). 5. Rauer A.E. Rhinoplastics. – In: Trudy pervoi moskovskoi oblastnoi konferentsii po chelyustno-litsevoi khirurgii. Moscow-Leningrad. 1936, pp.44-46 (In Russian). 6. Rosenfeld I.M. Destructuring the synechiae of nasal cavity appear-ing as a consequence of gun-shot wounds. Sverdlovsk, 1946. (In Russian). 7. Atkarskaya A.A. On physiology of paranasal sinuses. Zhutnal ushykh, nosovykh i gorlovykh boleznel. 1925; №5-6: 274-95 (In Russian). 8. Ulyanov Y.P. Nose aerodynamics. Arch. Otolaryngol. Head Neck Surg. 1995; 121: 352. 9. Ulyanov Y.P. A method of reconditioning the protective function of nose. Russian patent №009236. 10. Ulyanov Y.P., Polivanov P.P. Russian patents №№1,572,505 and 1,602,472.
|
||||
Fig. 1
|
Fig. 2
|
Fig. 3
|
||
|
|
||||
 |
Fig. 4
|
Fig. 5
|
Fig. 6
|
|
|
|
||||

