
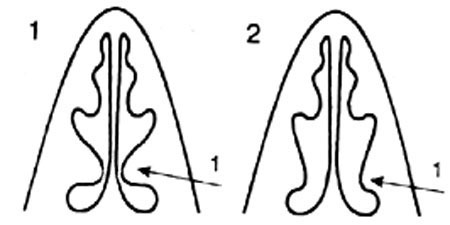
Fig. 1
Northern type of nasal aerodynamics is when the distance between the
anterior end of IT and the nasal septum is not more than 1.5-2 mm. :
Fig. 2
Southern type of nasal aerodynamics is when the distance between the
anterior end of IT and the nasal septum is more than 2.5 mm.:
1 - inferior turbinate is large in size .
1 - inferior turbinate is small in size .
NASAL AERODYNAMICS and RHINOSINUSITISES
Relationship between two parallel respiratory structures in the nose
The main cause of the night snoring is violations of the nasal aerodynamics
The functionality of the small ostiums of the nasal sinuses
VARIANTS OF NASAL AERODYNAMICS
NORMOGRAM OF NASAL AERODYNAMICS
PHYSIOLOGICAL BRIDGE REPRESENTED BY THE NASAL VALUE
SURGICAL RECONSTRUCTION OF NASAL AERODYNAMICS
SEPTOPLASRY UNDER CONTROL OF NASAL AERODYNAMICS
CONTRAINDICATION TO SEPTOPLASTY
PROTECTION OF THE INFERIOR NASAL PASSAGE FROM INSPIRATION
THE INSIDIOUSNESS OF THE UNILATERAL "SOUTHERN" NASAL AERODYNAMICS.
SNORING WHEN NASAL RESPIRATION IS SAVED.
"Northern" type of aerodinamics |
"Southern" type of aerodinamics |
 |
VARIANTS OF NASAL AERODYNAMICS(Uliyanov Y.P. Clinical manifestations the Variants of Nasal Aerodynamics. /Abstract/ Otolaryngology-Head and Neck Surgery -August 1998: V.119, N 2, 152-3.) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Objectives:Due to development of new devices, the study of the nasal aerodynamics has acquired an ever-increasing value, especially during recent years. This is accounted for by the fact that with the advent of a special device (Y.P.Ulyanov, P.P.Polivanov, 1988), it has become possible to examine separate air flows in the nasal passages both at inspiration and expiration, to establish the normogram of the nasal aerodynamics and to determine its two extreme variants: "the northern" and the "southern" (Y.P.Ulyanov, 1995, 1996, 1997). Patients with the "northern" type are better adapted to the harsh air of the mid-latitude temperate zone and probably therefore they catch a cold very seldom (once in 4-5 years). Persons with the "southern" type of aerodynamics are less protected in this aspect. They catch a cold regularly in autumn and winter more than once, forming the population of those disposed to epidemics of influenza. As a result, resistance of patients to acute rhinitis caused by common cold is in fact a qualitative criterion of efficiency of the protective properties of nasal aerodynamics. This correlation is especially clearly demonstrated after surgical reconstruction of the "northern" type of aerodynamics out of the "southern" one (Y.P.Ulyanov, 1997). The otherwise, after this surgical reconstruction of nasal aerodynamics the dry and subatrophic mucosa of nose becomes soft and moist without any signs of inflammation, and resistant to common colds of the wet seasons.METHODSTherefore at present, having at our disposal the extreme variants of the protective properties of nasal aerodynamics are as the criteria of their efficiency, we can examine all transitional forms and evaluate them from the clinical point of view. During endonasal rhinomanometry, we studies of nasal aerodynamics in 1000 patients with frequent fits of common cold and 300 practically healthy people facilitated detection of clinical manifestations of 2 extreme types of nasal aerodynamics, which had been observed previously by scientists. These are the "northern" type of nasal aerodynamics (NTA) and the "southern" type of nasal aerodynamics (STA). Using the principle of moving the main airstream at inspiration from MM to IM, patients were divided into 7 nasal aerodynamics groups, with airstream pressures differing from each other by 10 conditional units (CU) = 25 Pascal (Pa). MM at inspiration. Table 1. In Table 1, distribution of airstream at inspiration between IM and MM appears to be the main distinctive criterion of groups of patients with various values for nasal aerodynamics. The age range of patients was 2-86 years with a 1:1 male-to-female ratio. Clinical manifestations of different diseases in each of the nasal aerodynamic groups are marked with (+) to indicate less than 5% incidence, with (++) to indicate 6-10% incidence, and with (+++) to indicate incidence over 11%.RESULTS:Healthy patients adapted to average and northern latitudes made up 3 groups with 150-200 Pa entering MM at inspiration. Patients with regular seasonal colds were in 4 groups with airstream pressures of 50-125 Pa entering Apart from the detection of 2 extreme types of nasal aerodynamics, as the "northern" and "southern" type of nasal aerodynamics has been established and group of patients with complete equilibrium of the distribution of air flows between middle and inferior nasal passages (50 CU/50 CU). The patient of this group as and other three groups with 50-125 Pa (40 CU, 30 CU and 20 CU) had caught a cold frequently. At the same time, among the persons who were practically healthy and possess the "northern" type of aerodynamics there are two more groups with 150-200 Pa (60 CU and 70 CU)were well adapted to average and northern latitudes. The entry of the air flow through the superior nasal passage was approximately stable (10 CU in each group) and was not related to the distribution of air flows along the other nasal passages. As a result, 250 Pa (100 CU) were to go through the inferior and medial nasal passages. E.g., in the "southern" type of aerodynamics 20 CU go through the medial nasal passage, with 80 CU entering the inferior nasal passage. In patients with the "northern" type of aerodynamics, the situation was reverse, i.e. 80 CU go through the medial nasal passage, with 20 CU entering the inferior nasal passage. Clinical manifestations of these variants of distribution of the air flows were especially evident (Second part of Table 1). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The data of the Table demonstrate that appearance of rhinitis in directly depended upon the shift of the main air flow from the medial nasal passage to the inferior one. As long as the main air flow at inspiration entered through the medial nasal passage, patients caught a cold very seldom (once in 4-5 years), however, a slightest disturbance of this situation, be it only in 10 CU, with the distribution of air flows becoming an equal value (50/50), patients suffer from colds every year (up to twice a year). The further shift of the air flow to the inferior nasal passage increases the trend to two to three colds annually (with an additional 10 CU) and to four colds a year (with an additional 20 CU). However, further shift of the air flow to the inferior nasal passage (to 80 CU) causes a fifty-percent drop in the advent of seasonal cold of the superior respiratory ways, which suggests a contradiction to the above-mentioned trend and demands the further investigation. Therefore, we have carried out an additional analysis of correlations between clinical manifestations as related to the level of the shift of the air flow to the inferior nasal passage one. The leading place among the clinical manifestations is held by the subatrophic process of the mucosa of the nose, larynx and pharynx to be seen even in the group of healthy persons with 60 CU. Whereas a further shift of the air flow to the inferior nasal passage was causes the next increased subatrophic process with the maximum value to be reached in the persons with the "southern" type of nasal aerodynamics, when the atrophic process is already detected. The latter seems to be not so much evident in the "southern" nasal aerodynamics, so that the mucosa cannot probably respond with the protective inflammatory reaction in the form of acute rhinopharyngitis caused by seasonal colds with the occurrence rate being half as high. A false conclusion comes to mind that the atrophic process as if protects us from common cold. But is it so? It turns out that in this group of patients a deeper involvement of the inspiratory ways in the form of tracheobronchitis which occur less frequently as long as the air flow returns to the medial nasal passage, with a nearly complete disappearance when the equilibrium of the air flows is reached. Moreover, this group of patients suffer from fits of laryngospasms, and bronchial asthma, with the inflammatory process reaching even the lungs, often causing pneumonia. Therefore, excessive dryness of the mucosa of the superior inspiratory ways, while reducing the occurrence rate of acute seasonal rhinopharyngitis, lets the harsh air pass into the inferior inspiratory ways causing more severe diseases such as tracheobronchitis, bronchial asthma, and pneumonia, which is a further confirmation of the detected main trend. i.e. a correlation between the status of the inspiratory ways and the level of redistribution of the air flow at inspiration between the medial and inferior nasal passages, i.e. the evident protective properties of the nasal aerodynamics. This correlation is also corroborated by local clinical manifestations near the nose. Acute rhinitis is detected in groups with the air flow values at inspiration from 50 to 40 or 30 CU. Sinusitis is seen in groups with 50-40, 30 and 20 CU, with the following association taking place. The more pronounced mucosal atrophy is, the less frequently it occurs, but at the same time there is a risk of ozena. The reduced protective response of the mucosa with increased subatrophic process and appearance of atrophy is confirmed also by manifestations of vasomotor rhinitis which is so aggressive that affect even practically healthy persons in the group till 60 CU, but it occurs frequently also in the group with 30 CU, although it is not practically found in the group with 20 CU. Having studied certain correlations of the distribution of the air flow at inspiration, we cannot but take into account also the distribution of the air flow at expiration, as the latter affects the rate of compensatory influence of the warm and humid air flow on the mucosa of the inferior nasal passage damaged by the "harsh" air at inspiration. CONCLUSION:Clinical manifestations of reduction of the protective properties of nasal aerodynamics, such as frequent colds with local complications (eg, sinusitis, otitis, CR), occur in equal distribution of airstream between MM and IM. Further moving of the main airstream into IM on inspiration is accompanied by frequent colds and more serious complications with compromise of respiratory passageways, leading all the way to ozena, bronchial asthma, and pneumonia.REFERENCES:Uliyanov Y.P., Polivanov P.P. Russian patents ąą 1,572,505; 1,602,472,(1988). (In Russian).Uliyanov Y.P. Nose aerodynamics. Arch. Otolaryngol. Head Neck Surg. 1995; 121: 352 Uliyanov Y.P. Nose aerodynamics. Jor. Vrach, Moscow, 1996; 11: 39-40. (In Russian). Uliyanov Y.P. Method reconstruction of nasal aerodynamics. Jor. Vrach, Moscow,1997; 7: 31-33. (In Russian). Ulyanov Y.P. Normogram of nasal aerodynamics. XYI World Congr. Of Otolar. Head Neck Surg.(Sydney, Australia, 2-7 March, 1997: 1603-1607. Uliyanov Y.P. Surgical reconstruction of nasal aerodynamics. XYI World Congr. Of Otolar. Head Neck Surg.(Sydney, Australia, 2-7 March, 1997: 1591-1595. Uliyanov Yu. Clinical Medicine (Reference book of a practicing physician). MSPI, Moscow, 1997,V-2:1103 - 1152. (In Russian). Uliyanov Y.P. Relaytions bitween bronchial-pulmonary conditions and nasal aerodynamics. Vestnic of the Center of Endosurgery and Lithotripsy, Moscow, 1997; 1: 32-37. (In Russian).
  | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||