|
A new device, especially designed to analyze the actual developments of
the airflow in the nasal passages, was used in our studies, employing a technique
suggested by me (patents of the Russian Federation No. 1572505 and No. 1602472).
It proved possible to devise a graph of nasal aerodynamics in the following manner
for the first time.
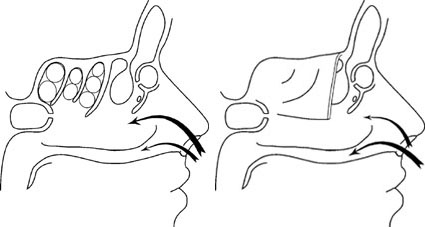
Inhaled air is divided in the nose into three streams of air passing through
the upper, median, and lower nasal passages. At the same time, 10 arbitrary units of
air flow through the upper passage, 80 units through the median, and 20 units through
the lower passage. This distribution of airflow moistens and warms the air in the median
and upper nasal passages wherein all paranasal sinuses open, with the latter washed by
the airstream at inhalation. Owing to a lack of sinuses, the airstream flowing through
the lower passage does not face similar treatment; consequently, the mucous membrane of
the lower nasal passage bears the brunt of desiccating and cooling air. However, the
excess capacity borne by the mucous membrane of the lower nasal passage is offset by the
warm humidified air at exhalation, constituting 80 arbitrary units of airflow. The
distribution of air at exhalation in the median and upper nasal passages amounts to 20
and 10 arbitrary units, respectively.
A protection of the mucous membrane of the upper respiratory passageways
in such a manner is particularly important in the dry cool environment of the midlatitude
temperate zone and steppe regions, where the indigenous population has evolved a natural
protective aerodynamic mechanism. Residents of the warm humid climatic zones have evidently
not formed such a mechanism. Consequently, the main airstream is drawn in through the
lower nasal passage at inhalation and expelled through the median nasal passage at
exhalation, reaching 80 arbitrary units in the process. People with southern nose
aerodynamics are characterized by less developed turbinal bones.
Another special feature has come to light. While aerodynamics of the northern
type nose do not have an ad-verse effect in warm humid climatic conditions, aerodynamics
of the southern type are ill suited for more northern latitudes with their dry cool
climate.
As the main airstream of people with southern nose aerodynamics passes
through the lower nasal passage at inhalation, devoid of communication with the paranasal
sinuses, air enters the upper respiratory passageways, as if it were "untreated."
Consequently, it exerts a highly desiccating and cooling effect on the mucous membranes
of the lower passages, pharynx, larynx, trachea, and bronchi, thereby causing subsequent
chronic inflammation. As this occurs, the lower nasal passage undergoes the most strain,
as the main airstream at exhalation is directed into the median nasal passage, leaving the
mucous membrane of the lower nasal passage virtually unprotected. This is conducive to
frequent common colds, chronic rhinitis, vasomotor rhinitis, and afflictions of the
accessory sinuses. The mucous membrane the pharynx in such individuals appears subatrophic
and dry, and this may result in chronic pharyngitis. The mucous membrane of the larynx
also dries up, causing chronic subatrophic and atrophic laryngitis, thereby placing a
severe strain on the vocal cords and even disabling people whose voices are the linchpins
of their professions, eg. singers, radio and television announcers, and teachers. The
drying up of the mucous membrane of the trachea and bronchi could cause chronic
tracheobronchitis, asthmatic bronchitis, and other ailments. Moreover, the number of
such individuals far exceeds the number of migrants from southern regions, as the nasal
aerodynamics of the southern type are, owing to its age, very prevalent, inherited down
to the fifth or 10th generation. Consequently, many seemingly native residents of the
middle latitudes have nasal aerodynamics of the southern type or its transitional forms.
When these people fall ill. the usual symptomatic treatment proves of little
help, as the individual specifics of their nasal aerodynamics are ignored.
Exceptionally good results have been obtained using the plastic surgery
modality to transform nose aerodynamics into its northern counterpart. The otherwise dry
and subatrophic mucous membrane of the nose and laryngeal pharynx becomes, after the
restoration of the protective mechanism, soft and moist and breathes freely. People
dependent on their voices are able to go about their professions with ease. The incidence
of common cold disorders and cases of sick leave are consequently drastically reduced.
Chronic tracheobronchitis is also amenable to more effective treatment in this case.
|